01 December 2022: Clinical Research
Clinical Outcomes of Extracranial Carotid Artery-Related Stroke Eligible for Mechanical Reperfusion on Top of Per-Guidelines Thrombolytic Therapy: Analysis from a 6-Month Consecutive Patient Sample in 2 Centers
Karolina Dzierwa 12ABDEF* , Magdalena Knapik 234ABDEF , Łukasz Tekieli 235ABDEF , Adam Mazurek 23ABDEF , Małgorzata Urbańczyk-Zawadzka 26BCD , Artur Klecha 7ABD , Tomasz Kowalczyk 7ABD , Teresa Koźmik 7ABD , Łukasz Wiewiórka 2567ABD , Paweł Banyś 6BCD , Ewa Węglarz 25BC , Justyna Stefaniak 8CD , Rafał T. Nizankowski 9ADF , Iris Q. Grunwald 1011ADEF , Piotr Musiałek 23ABCDEF*DOI: 10.12659/MSM.938549
Med Sci Monit 2022; 28:e938549
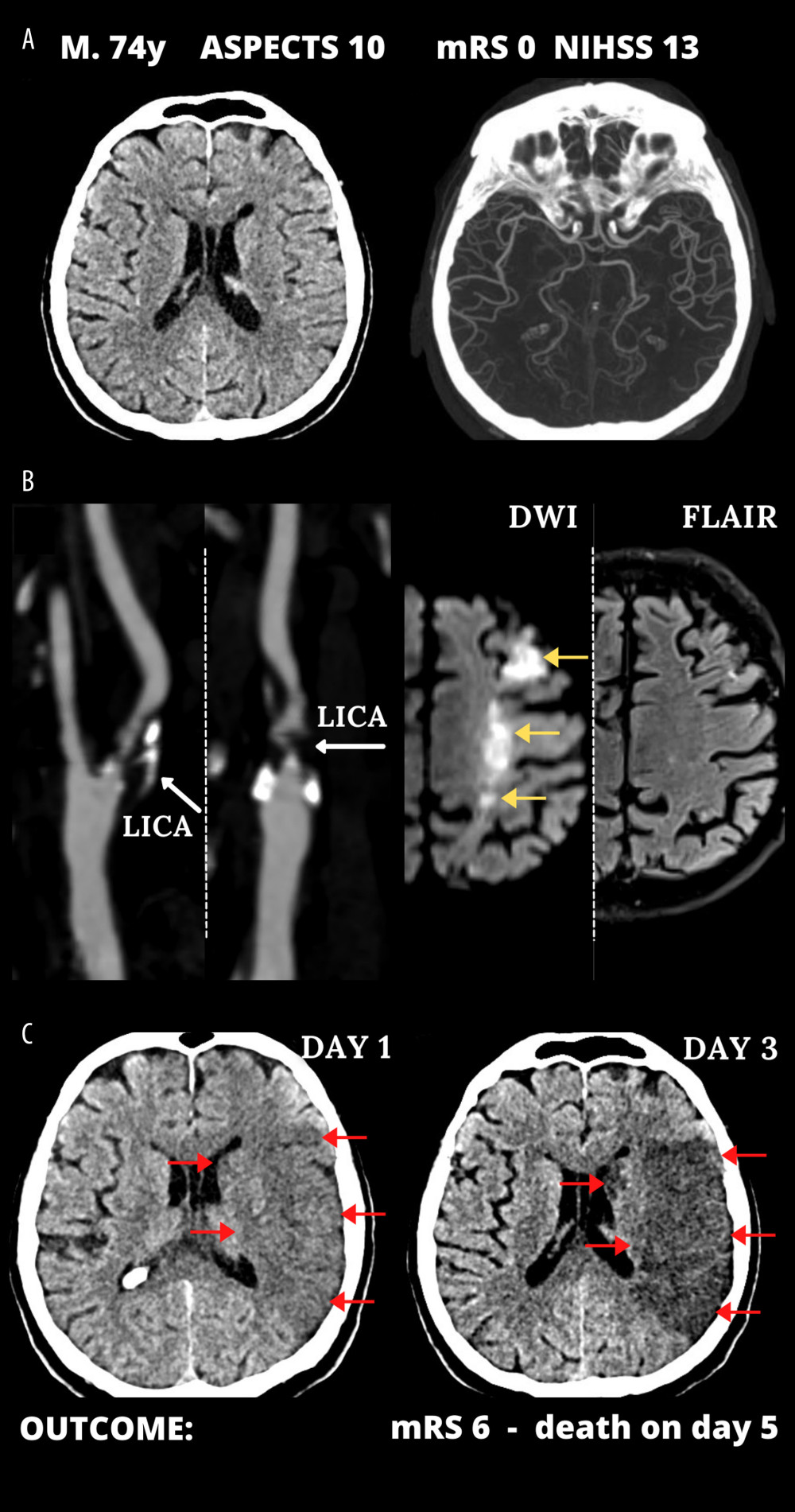
Figure 1 Typical cerebral infarct evolution in an acute ischemic stroke of the carotid artery origin in emergency mechanical reperfusion (EMR) eligible patient that did not receive EMR (EMR-untreated). (A) Admission cerebral computed tomography (day 0) was normal; Alberta Stroke Program Early Computed Tomography Score (ASPECTS) 10 in a man presenting with left hemispheric stroke symptoms of increasing severity National Institutes of Health Stroke Scale (NIHSS) – 13 (left) and computed tomography angiography showed no intracranial artery occlusion and good collaterals (Tan 3) (right). (B) Sub-occlusive left internal carotid artery (LICA) stenosis (left); magnetic resonance imaging demonstrated potentially reversible hyperacute left-sided diffusion restriction on diffusion-weighted imaging (DWI, yellow arrows) which are absent on the fluid-attenuated inversion recovery (FLAIR) sequence (right). IV thrombolysis was started, and the patient was observed for thrombolysis effect; there was no referral for EMR. Neurologic status gradually deteriorated. (C) Large cerebral tissue loss (red arrows) seen on control computed tomography 12 hours after 1st scan (left, thrombolysis ineffective, collateral supply exhaustion) and on day 3 (right). Figure was created with the use of Canva (Perth, Australia).