04 April 2024: Clinical Research
Outcomes of Chengdu Pediatric Emergency Triage Criteria: A Retrospective Study of 198,628 Pediatric Patient Records
Jing Zhao12BCE, Yingying Zhao12BC, Juan Hu12ABCEG*, Yan Huang12BE, Liqing He12BDOI: 10.12659/MSM.942814
Med Sci Monit 2024; 30:e942814






Abstract
BACKGROUND: The Chengdu pediatric emergency triage criteria were developed at our hospital and consist of 4 triage levels: immediate treatment (level 1), treatment within 10 min (level 2), treatment within 30 min (level 3), and treatment within 240 min (level 4). This study aimed to evaluate outcomes from the levels 1 to 4 of this triage criteria.
MATERIAL AND METHODS: A self-designed survey form was used to collect pediatric Emergency Department (ED) patients’ general data, including age, sex, and chief concern, and clinical data, including triage level, whether the patient had died, and whether the patient was admitted to our hospital. A total of 198,628 patient records that were triaged during January to May 2022 using Chengdu pediatric emergency triage criteria were included in this retrospective study. The numbers of patients triaged to levels 1, 2, 3, and 4 were 128, 1164, 14,560, and 182,776, respectively.
RESULTS: Statistically significant differences were found in waiting time for treatment, hospital admission rates, admission conversion rates, and case mix index at admission under different triage levels. The higher the triage priority level, the shorter the waiting time for ED treatment, higher the hospital admission and admission conversion rates, and higher case mix index value.
CONCLUSIONS: The Chengdu pediatric emergency triage criteria developed and applied within our hospital appears to be characterized by good clinical validity. Equipped with this triage criteria, triage nurses are more capable of determining the severity and emergency of the pediatric ED patients’ health conditions and effectively triaging the patients.
Keywords: Emergency Service, Hospital, Pediatrics, Triage
Introduction
In pediatric emergency medicine, triage is a key step in the alleviation of Emergency Department (ED) crowding that takes into account the severity and urgency of patients’ health conditions. Its aim is to rationally allocate medical resources and identify which treatment and nursing methods are the most appropriate during resource restrictions. Triage accuracy is associated with the quality of treatment and care provided to patients [1]. Triage is an essential practice owing to the acute onset and seasonality of pediatric diseases and potentially excessive numbers of pediatric patients being admitted to hospital during “peak season” [2]. Owing to the limited capacity of outpatient registration and lack of nighttime outpatient service, patients who cannot be registered in the Outpatient Department will enter the ED, leading to ED crowding [3]. Pediatric patients’ parents hope their children receive timely treatment and often make pressing demands for emergency nursing, thereby adding to the stress experienced by pediatric emergency triage nurses. In the previous survey of our hospital’s emergency nurses’ degree of willingness in carrying out their responsibilities, we found that triage received the lowest score.
Our hospital’s emergency triage decisions have been formed through the following stages: the triage nurse’s own knowledge and experience; the triage criteria for adults; and, the Chinese and foreign countries’ pediatric emergency triage criteria. Our hospital’s triage recording system has evolved through 3 stages: manual registration, electronic medical record entry, and then the current electronic triage system. In December 2020, a pediatric emergency triage criteria suitable for our hospital, called the Chengdu pediatric emergency triage criteria, was developed at our hospital using the Delphi method. This triage criteria were informed by internationally recognized triage criteria, such as the Emergency Severity Index and Canadian Triage Acuity Scale, as well as the pediatric emergency triage criteria used in some hospitals in China. Chengdu pediatric emergency triage criteria is a 4-level triage tool. Its maximum waiting time for treatment under different triage levels are as follows: level 1, immediate treatment; level 2, within 10 min; level 3, within 30 min; and level 4, within 240 min (Table 1) [4]. The reliability and validity of the Chengdu pediatric emergency triage criteria was verified in 2021 [5]. This retrospective study included 198 628 patient records that were triaged between January and May 2022 using the Chengdu pediatric emergency triage criteria and aimed to evaluate outcomes from levels 1 to 4 of this triage criteria.
Material and Methods
ETHICS APPROVAL:
This study was conducted in accordance with the Declaration of Helsinki. All research methods were conducted in accordance with the relevant guidelines and regulations. This study was approved by the Medical Ethics Committee of West China Second University Hospital, Sichuan University (2022 Medical Scientific Research for Ethical Approval No. 138). Because this was a retrospective study based on patient records, the Medical Ethics Committee of West China Second University Hospital, Sichuan University approved the waiver of informed consent in this study.
STUDY DESIGN:
A total of 198 628 records of cases that were triaged in the ED of our hospital during January to May 2022 using the Chengdu pediatric emergency triage criteria were included in this study (level 1: 128 cases; level 2: 1164 cases; level 3: 14 560 cases; and level 4: 182 776 cases).
A self-designed survey form was used to collect pediatric ED patients’ general data, including age, sex, and chief concern, and clinical data, including triage level, whether the patient had died, whether the patient was admitted to our hospital, case mix index (CMI) at admission, and waiting time for treatment in the ED. The above-mentioned data were extracted from our hospital’s health information system. Data accuracy was checked by multiple researchers, and data entry was checked by 2 researchers to ensure appropriate integrity and accuracy of data.
QUALITY CONTROL:
Our hospital’s triage research group developed the Chengdu pediatric emergency triage guidelines and criteria and have conducted relevant training for triage nurses, including point-by-point explanation, case analysis, and situational simulation, so that the triage nurses could thoroughly understand the triage criteria and pass the relevant examination. The research group members provided follow-up guidance for triage nurses within the first month after the triage criteria were put into service to ensure triage nurses’ correct manipulation of the triage criteria. Each triage nurse at our hospital must possess at least 3 years of ED work experience before being permitted to work independently in the triage position.
STATISTICAL ANALYSIS:
SPSS 23.0 was used for statistical analysis. Measurement data were presented as mean±standard deviation. Enumeration data were expressed in the forms of frequency and component ratio. The chi-square test was used to compare the waiting times for treatment and hospital admission rates under different triage levels.
Results
PATIENTS’ GENERAL DATA:
A total of 198 628 patients visited the ED during January to May 2022. Patients’ general data are presented in Table 2.
COMPARISON BETWEEN TRIAGE LEVELS AND WAITING TIME FOR TREATMENT:
The Kruskal-Wallis H test results show that statistically significant differences existed between the different triage levels and the waiting time for treatment (P=0.000). The Kruskal-Wallis one-way analysis of variance results showed that no statistically significant difference existed between patients triaged to levels 1 and 2 (P=0.420), whereas statistically significance differences existed between patients triaged to other levels (P=0.000; Tables 3, 4).
COMPARISON BETWEEN TRIAGE LEVELS AND HOSPITAL ADMISSION RATES:
The chi-square test results showed a statistically significant difference between triage levels and hospital admission rates (P=0.000). The pairwise comparison results showed the hospital admission rate of patients triaged to level 1 was higher than the rates of patients triaged to levels 2, 3, and 4; the hospital admission rate of patients triaged to level 2 was higher than that of patients triaged to levels 3 and 4; and, the hospital admission rate of patients triaged to level 3 was higher than that of patients triaged to level 4. In summary, statistically significant differences were found between hospital admission rate by triage level (P<0.05; Tables 5, 6).
COMPARISON BETWEEN TRIAGE LEVELS AND ADMISSION CONVERSION RATES:
For the patients triaged to different levels, the chi-square test results showed that statistically significant differences existed between the admission conversion rates (proportion of patients receiving hospital admission letters and accepting admission; P=0.000). Among the patients who were triaged to levels 1 and 2 and received hospital admission letters, the pairwise comparison results showed no statistically significant difference in the admission conversion rates between them (P=0.994); by contrast, the admission conversion rates of patients triaged to levels 1 and 2 were higher than those of the patients triaged to levels 3 and 4, and the admission conversion rate of patients triaged to level 3 was higher than that of patients triaged to level 4. In summary, statistically significant differences were found between admission conversion rate by triage level (P=0.000) (Tables 7, 8).
COMPARISON BETWEEN TRIAGE LEVELS AND CMI VALUES AT ADMISSION:
The Kruskal-Wallis H test results showed that statistically significant differences existed between the CMI values at admission in the patients at different triage levels (P=0.000). The Kruskal-Wallis one-way analysis of variance results showed that no statistically significant differences existed between CMI values either in patients triaged to levels 1 and 2 (P=0.360) or in patients triaged to levels 3 and 4 (P=0.463). However, statistically significant differences existed in CMI values at admission between patients triaged to other triage levels (P<0.05) (Tables 9, 10).
Discussion
LIMITATIONS:
It should be noted that this study was conducted in the ED of only a single grade A tertiary hospital in China. A multi-center study is needed to further evaluate the outcomes using the triage criteria. Moreover, the criterion-related validity indicators selected for this study were insufficient; further predictive research should consider other variables, including death rate, Pediatric Intensive Care Unit admission, and the provision of medical resources on site. More criterion-related validity indicators should be included to further test the outcomes using the triage criteria.
Conclusions
The Chengdu pediatric emergency triage criteria developed and applied within our hospital appears to be characterized by good validity. Equipped with this triage criteria, triage nurses are more capable of determining the severity and emergency of the pediatric ED patients’ health conditions and effectively triaging the patients. Internationally recognized triage tools generally consist of comprehensive triage implementation guidelines. However, to improve the suitability of Chengdu pediatric emergency triage criteria, the triage criteria should be refined and, where appropriate, corresponding implementation guidelines should be imported.
Tables
Table 1. Chengdu pediatric emergency triage criteria.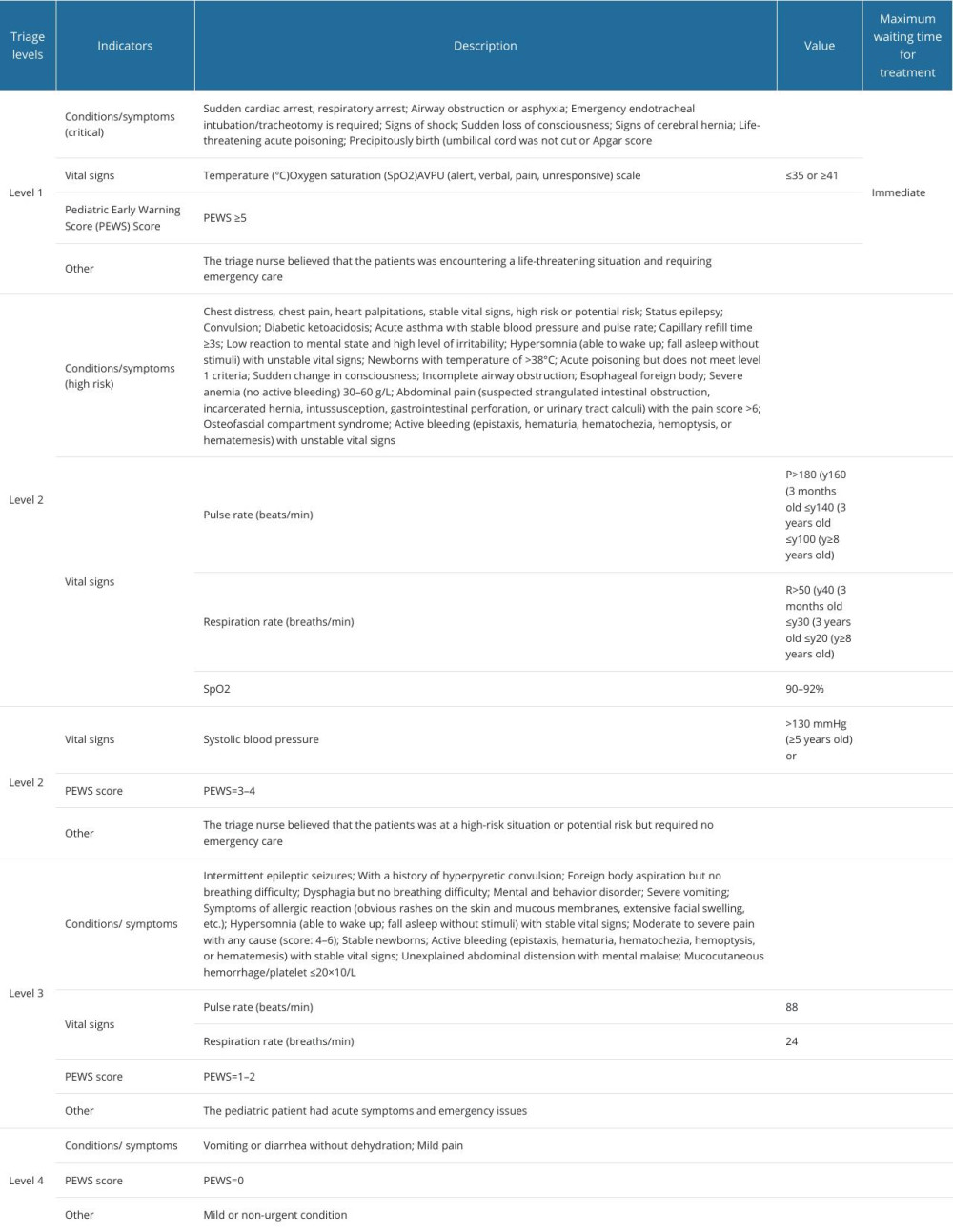 Table 2. Patients’ general data.
Table 2. Patients’ general data.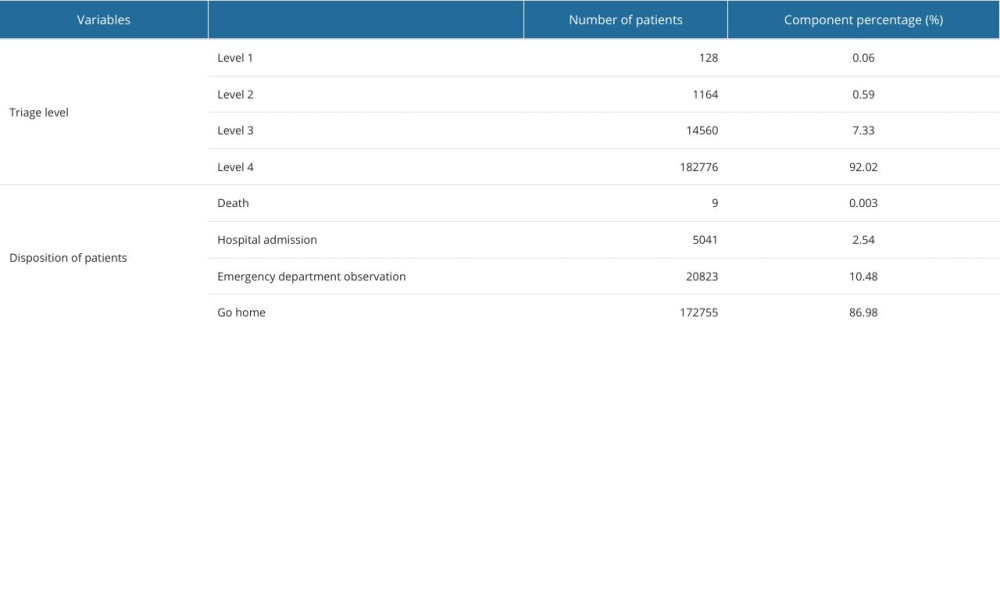 Table 3. Comparison between triage levels and waiting time for treatment.
Table 3. Comparison between triage levels and waiting time for treatment.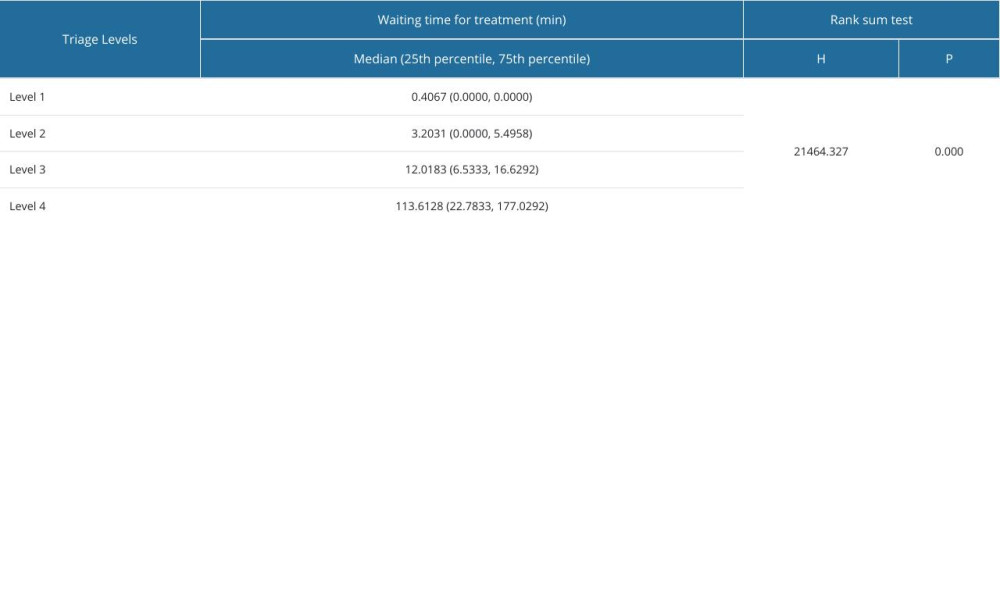 Table 4. Pairwise comparison of waiting time for treatment between different triage levels.
Table 4. Pairwise comparison of waiting time for treatment between different triage levels.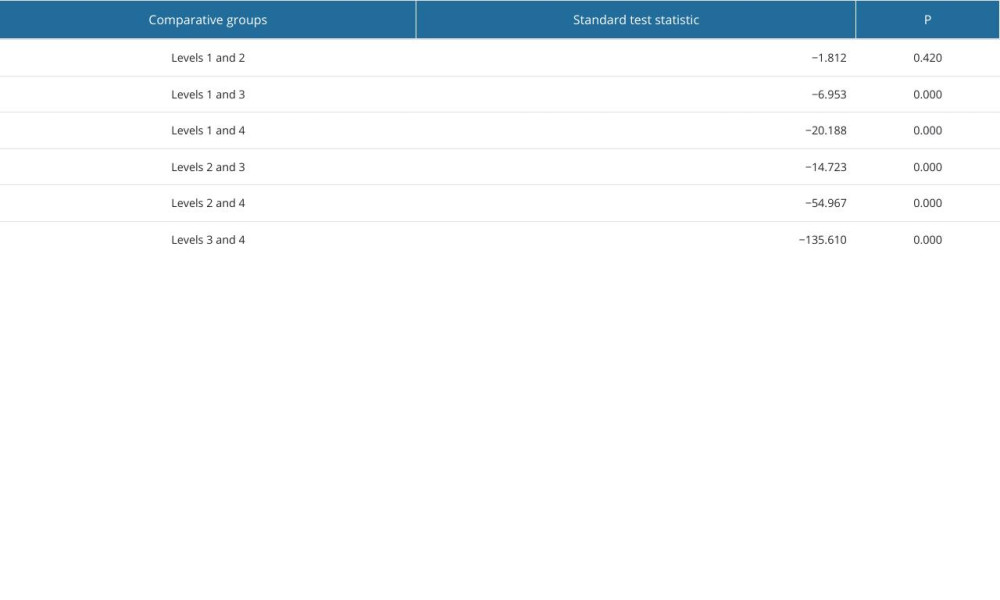 Table 5. Comparison between triage levels and hospital admission rates.
Table 5. Comparison between triage levels and hospital admission rates.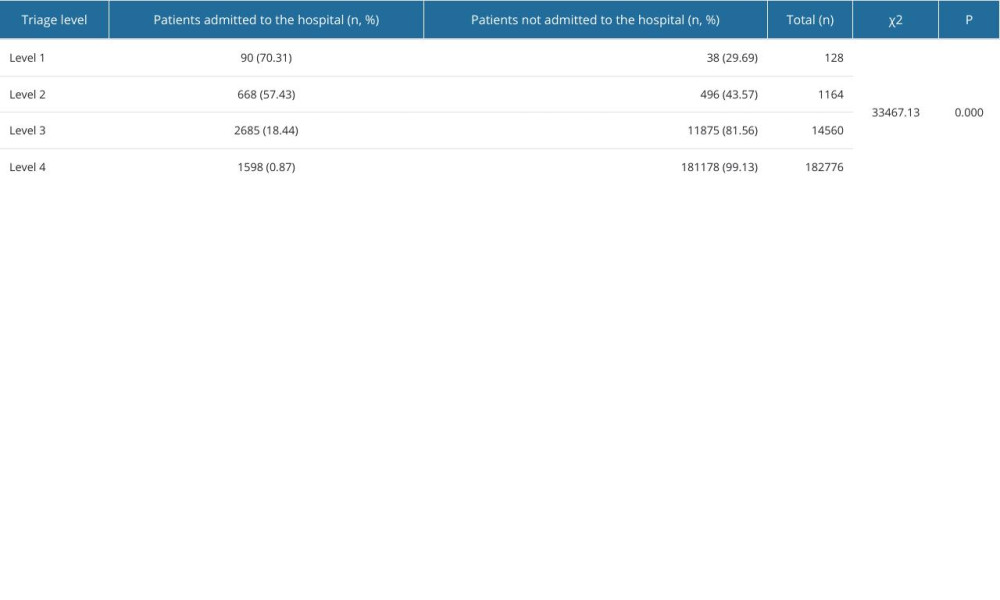 Table 6. Pairwise comparison of hospital admission rates between different triage levels.
Table 6. Pairwise comparison of hospital admission rates between different triage levels.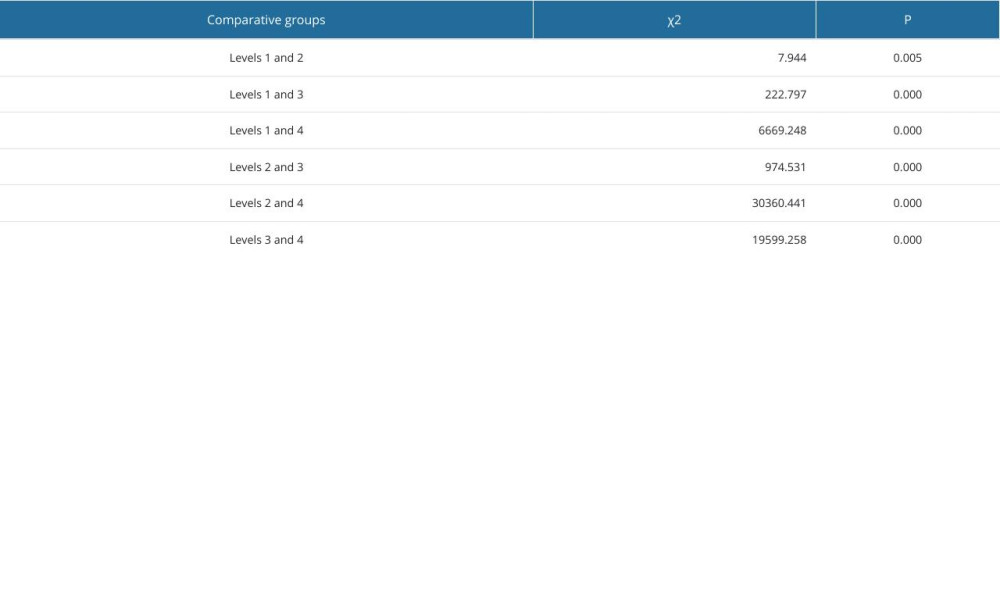 Table 7. Comparison between triage levels and admission conversion rates.
Table 7. Comparison between triage levels and admission conversion rates.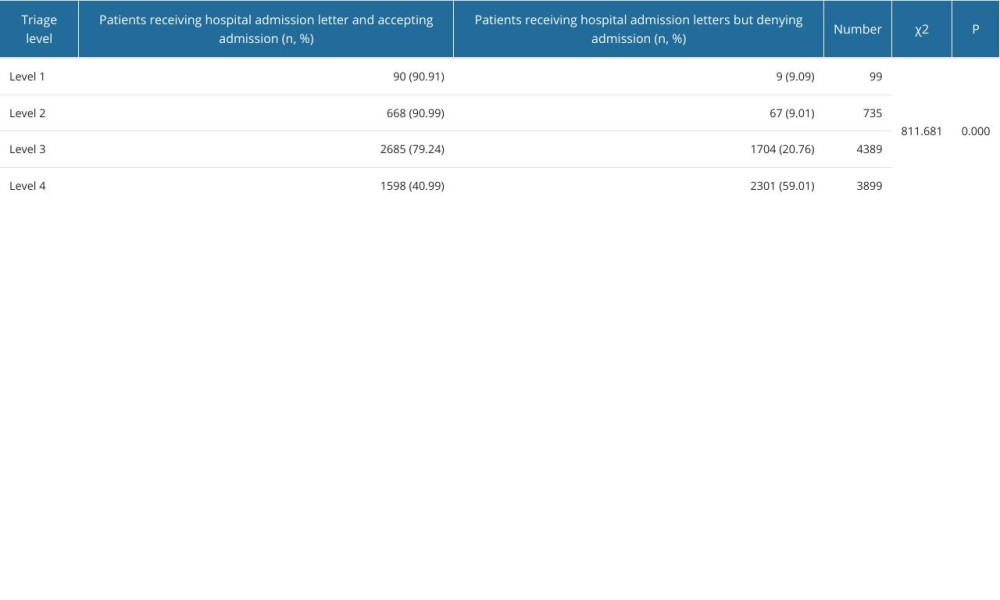 Table 8. Pairwise comparison of admission conversion rates between different triage levels.
Table 8. Pairwise comparison of admission conversion rates between different triage levels.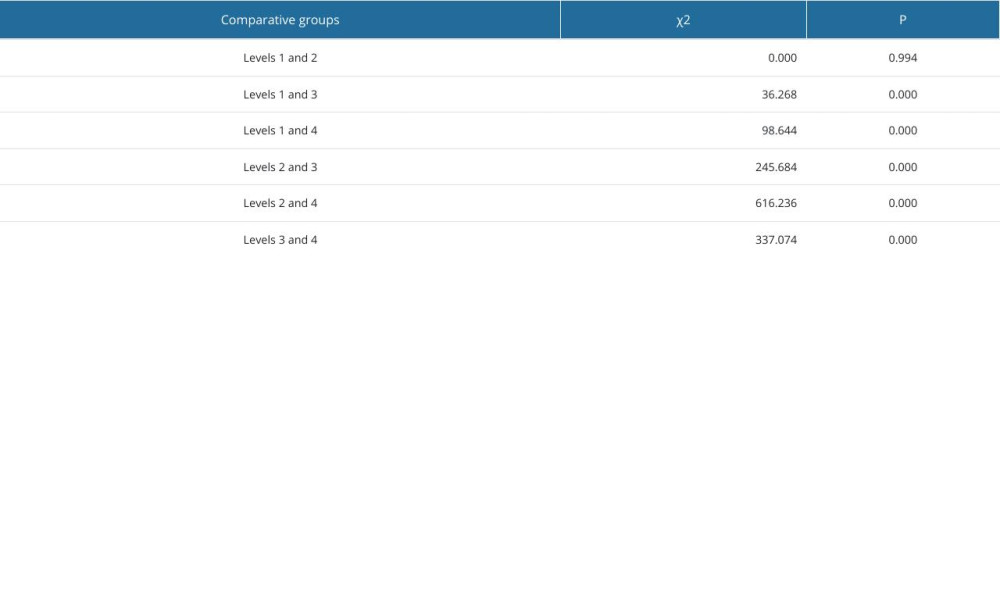 Table 9. Comparison between triage levels and care mix index values at admission.
Table 9. Comparison between triage levels and care mix index values at admission.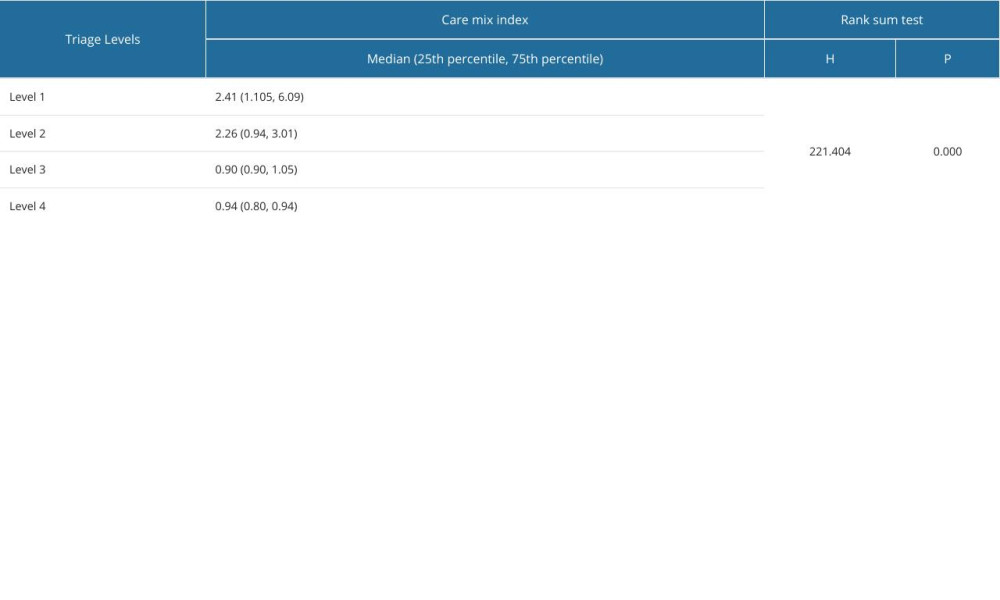 Table 10. Pairwise comparison of care mix index values at admission between patients triaged to different levels.
Table 10. Pairwise comparison of care mix index values at admission between patients triaged to different levels.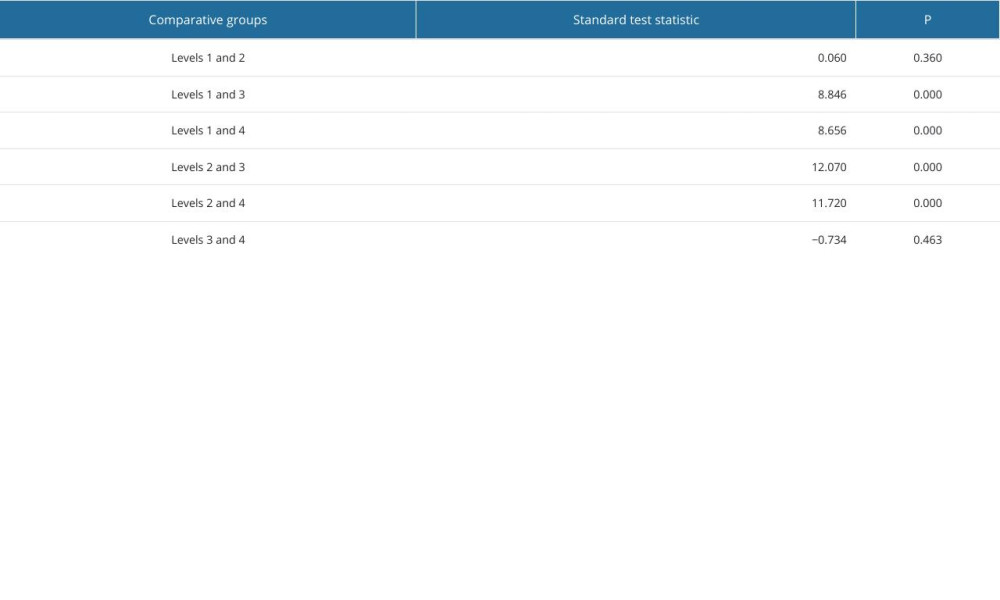
References
1. Tam HL, Chung SF, Lou CK, A review of triage accuracy and future direction: BMC Emerg Med 20, 2018; 18(1); 58
2. Ren J, Guo X, Xu SStudy on the change trend and flow of emergency department visits of a tertiary hospital in Xinjiang from 2018 to 2021: Chinese Journal of Hospital Statistics, 2023; 30(5); 391-95 [in Chinese]
3. Gao XThe research on the current situation of outpatient treatment and its resource optimization in a class 3A children’s hospital, 2017, Chongqing (China), Chongqing Medical University [in Chinese]
4. Zhao Y, He L, Hu J, Using the Delphi method to establish pediatric emergency triage criteria in a grade A tertiary women’s and children’s hospital in China: BMC Health Serv Res, 2022; 22(1); 1154
5. Zhao Y, He L, Hu J, Using the Delphi method to establish pediatric emergency triage criteria in a grade A tertiary women’s and children’s hospital in China: BMC Health Serv Res, 2022; 22(1); 1154
6. Zhang C, Zhou YAnalysis on errors regarding content validity index used in evaluation of measurement tools in Chinese nursing literature: Journal of Nursing Science, 2020; 35(4); 86-88 [in Chinese]
7. Chen Q, 2017, Fuzhou (China), Fujian Medical University [in Chinese]
8. Huang X, Guo AUse and evaluation of internationally recognized emergency triage criteria: Chinese Journal of Nursing, 2014; 49(5); 597-601 [in Chinese]
9. Ng CJ, Yen ZS, Tsai JC, Validation of the Taiwan triage and acuity scale: A new computerised five-level triage system: Emerg Med J, 2011; 28(12); 1026-31
10. Fu R, Jin J, Huang GStudy on the application of pediatric emergency triage scale: Chinese Journal of Emergency and Critical Care Nursing, 2020; 1(5); 402-4 [in Chinese]
11. Campos-Gómez X, Martínez-Lara N, Juncos-Moyano A, Yock-Corrales A, Validation of the Pediatric Canadian Triage and Acuity Scale at the emergency department of a tertiary children’s hospital in Costa Rica: Cureus, 2021; 13(7); e16191
12. Zhiting G, Jingfen J, Shuihong C, Reliability and validity of the four-level Chinese emergency triage scale in mainland China: A multicenter assessment: Int J Nurs Stud, 2020; 101; 103447
13. Ødegård SS, Tran T, Næss-Pleym LE, Risnes K, Døllner H, A validity study of the rapid emergency Triage and treatment system for children: Scand J Trauma Resusc Emerg Med, 2021; 29(1); 18
14. Souza CC, Araújo FA, Chianca TCScientific literature on the reliability and validity of the Manchester Triage System (MTS) protocol: A integrative literature review: Rev Esc Enferm USP, 2015; 49(1); 144-51 [in Portuguese]
15. Ganapathy S, Yeo JG, Thia XHM, The Singapore Paediatric Triage Scale validation study: Singapore Med J, 2018; 59(4); 205-9
16. Hansoti B, Jenson A, Keefe D, Reliability and validity of pediatric triage tools evaluated in Low resource settings: A systematic review: BMC Pediatr, 2017; 17(1); 37
17. Ding L, Zuo A, Jiang G, Li HThe connotation and application of case combination index: Chinese Health Quality Management, 2022; 29(7); 58-61 [in Chinese]
18. Aeimchanbanjong K, Pandee U, Validation of different pediatric triage systems in the emergency department: World J Emerg Med, 2017; 8(3); 223-27
Tables
Table 1. Chengdu pediatric emergency triage criteria.Table 2. Patients’ general data.Table 3. Comparison between triage levels and waiting time for treatment.Table 4. Pairwise comparison of waiting time for treatment between different triage levels.Table 5. Comparison between triage levels and hospital admission rates.Table 6. Pairwise comparison of hospital admission rates between different triage levels.Table 7. Comparison between triage levels and admission conversion rates.Table 8. Pairwise comparison of admission conversion rates between different triage levels.Table 9. Comparison between triage levels and care mix index values at admission.Table 10. Pairwise comparison of care mix index values at admission between patients triaged to different levels. In Press
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
11 Mar 2024 : Clinical Research
Enhancement of Frozen-Thawed Human Sperm Quality with Zinc as a Cryoprotective AdditiveMed Sci Monit In Press; DOI: 10.12659/MSM.942946
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952