06 May 2024: Clinical Research
Tissue Inhibitors of Metalloproteinase 1 (TIMP-1) and 3 (TIMP-3) as New Markers of Acute Kidney Injury After Massive Burns
Wojciech KlimmDOI: 10.12659/MSM.943500
Med Sci Monit 2024; 30:e943500






Abstract
BACKGROUND: Acute kidney injury (AKI) is a common and serious complication after massive burn injury. One of the postulated etiologies is destruction of the extracellular matrix of nephrons, caused by a local imbalance between matrix metalloproteinases (MMPs) and specific inhibitors. The aim of this study was to analyze the dynamics of tissue inhibitors of metalloproteinases (TIMPs) during the first 5 days after massive thermal injury and the relationship with the risk of AKI.
MATERIAL AND METHODS: Thirty-three adults (22 men, 11 women) with severe burns were enrolled in the study. The values of TIMPs 1 to 4 were measured in blood serum and urine using the multiplex Luminex system. The associations between TIMPs and the risk of AKI were analyzed by using the generalized linear mixed models for repeated measurements.
RESULTS: Significant changes in serum and urine activities of TIMPs were confirmed, especially during the first 2 days after burn injury. Almost half of patients presented renal problems during the study. Significant differences between values of TIMPs in AKI and non-AKI status were also observed. However, a significant relationship between concentration of TIMPs and risk of AKI was confirmed only for urine TIMP-1 and serum TIMP-3.
CONCLUSIONS: The evaluation of TIMPs in the early stage after burn injury has potential benefits. The important roles of urine TIMP-1 and serum TIMP-3, as novel markers of the risk of AKI development, were confirmed. Other parameters require further analysis.
Keywords: Burn Units, Acute Kidney Injury, Matrix Metalloproteinase Inhibitors, TIMP2 Protein, Human, TIMP1 Protein, Human
Introduction
Acute kidney injury (AKI) is one of the components of burn injury. This frequent and serious complication of massive thermal trauma typically occurs during the first few days after a burn. AKI worsens the clinical course and patient survival. Diagnostic methods for this complication are currently insufficient, and the factors responsible for its evolution are not entirely understood [1].
A possible cause of AKI is the increase of activity of pro-inflammatory factors inside the renal parenchyma, which are released from thermally injured tissue [2]. Cytokines released into the bloodstream can damage the extracellular matrix (ECM) inside the nephrons by inducing specific proteolytic enzymes, for example, matrix metalloproteinases (MMPs). Lysis of support proteins and intracellular fibers and disintegration of renal interstitium structure occur. Vascular endothelial alterations cause the collapse of the vascular loop and acute ischemia among functional nephrons, ultimately leading to acute renal failure [3–5].
In response to severe inflammation and renal parenchyma ischemia, biologically active factors are locally induced to reduce destruction of nephrons and initiate repair processes. However, a consequence of rapid perfusion restoration is the risk of releasing accumulated toxic factors and developing acute ischemia-reperfusion injury in renal parenchyma and tubular damage [6].
MMPs are zinc atom-containing proteolytic enzymes, whose primary function is participating in the reconstruction and degradation processes of ECM elements [7]. Increased activity of MMPs is often observed during AKI and can be a poor prognostic factor for the recovery of kidney physiological functions, potentially worsening patient outcomes [8–10]. The precise impact of MMPs on the function of nephrons during AKI has not yet been sufficiently investigated. Researchers do not agree on the role of MMPs and suggest they may play a part in both renal parenchyma injury and protection and repair processes [11–13].
Activity of MMPs is strictly controlled by specific tissue inhibitors of metalloproteinases (TIMPs), which prevent their excessive accumulation in the ECM and disruption of its structure. In normal physiological conditions, MMPs and TIMPs are mutually inhibited in a negative feedback mechanism that maintains ECM reconstruction in a balance between absorption and synthesis [14]. So far, 4 types of TIMPs have been identified, TIMP-1-4, which regulate the activity of various MMPs [15].
AKI and burn injury can modify the serum and urine concentrations of TIMPs [16]. The etiology of this phenomenon is not well understood, but it is likely related to the protection and repair processes within the structures of injured organs. This can be caused by the inhibition of the destructive impact of secreted endopeptidases, blocking of active MMP forms, and restoration of the physiological equilibrium between the activity of MMPs and TIMPs [17,18].
The aim of this study was to evaluate the dynamics of the activities of TIMPs in blood serum and urine in patients during the first days after massive thermal injury and their impact on the risk of early phase of AKI occurrence.
Material and Methods
STUDY GROUP:
In this prospective project, the study group was recruited from adult patients hospitalized in a specialist burn unit. The basic criteria for inclusion in the study group was an isolated massive thermal injury of second or third degree covering at least 30% of the total body surface area (TBSA) or at least 20% TBSA with an associated respiratory tract burn, which occurred no more than 72 h before hospitalization. Patients with other causes of burn injury, such as chemical burn and sunburn, mixed injuries connected with crush accidents, such as after explosions, and multi-organ traumas, such as broken bones or craniocerebral injuries, were also excluded. Histories of serious chronic renal, pulmonary, or cardiac dysfunction and active infections were also disqualifying criteria. According to the project protocol, patients were initially recruited during their primary hospitalization at the emergency ward and then evaluated by project team members in the participating clinical department. At the time of hospitalization, vital signs, level of consciousness using the Glasgow scale, and the severity of the burn, using the Abbreviated Burn Severity Index, were assessed.
Following the directions of the project, a unified treatment with high-volume fluid resuscitation was introduced at the time of hospital admission. During hospitalization, each patient was treated in accordance with current standards [19]. Fluid balance and volume status were strictly controlled throughout the observation period using objective diagnostic techniques, such as central venous pressure measurement and hematocrit range. In each patient, vital signs were evaluated, with special consideration given to fluid balance and daily urine collection.
AKI DIAGNOSTICS:
In accordance with the objectives of the project, the following renal function parameters were estimated: blood serum urea (sUrea) and creatinine (sCr) concentrations, estimated glomerular filtration rate (eGFR), and hourly and daily diuresis. The diagnosis of AKI was based on the Acute Kidney Injury Network criteria and Risk, Injury, Failure, Loss of function, End-stage kidney disease (RIFLE) classification. In each patient, the current AKI status of the day was computed in the morning hours, along with other biochemical parameters. AKI-positive status was assigned to the appropriate RIFLE stages. The observation time was the first 5 days of hospitalization.
DETERMINATION OF TIMPS:
To implement the project assumptions, TIMP-1-4 values in blood serum (sTIMP-1-4) and TIMP-1-2 values in urine (uTIMP-1-2) were determined in the first 5 days of hospitalization in the morning hours. Serum and urine were prepared by centrifugation and stored at −80°C until being analyzed in a single batch.
COLLECTION AND STORAGE OF SERUM AAMPLES:
Serum separator tubes were used and allowed blood samples to clot for 30 min at room temperature before centrifuging them for 15 min at 1000×g. Serum was removed immediately, and aliquots were stored at −80°C.
COLLECTION AND STORAGE OF URINE SAMPLES:
The urine (mid-stream) samples were aseptically collected, voided directly into a sterile container, and centrifuged to remove particulate matter. Aliquots were stored at −80°C.
DESCRIPTION OF THE METHODS USED FOR TIMP DETERMINATION:
On the day of the assay, all previously frozen serum samples were centrifuged at 16 000×g for 4 min immediately prior to use and diluted 50 times with test calibrator diluents. The urine samples were diluted 5 times with the same calibrator. The concentrations of TIMP-1-4 in serum and TIMP-1-2 in urine were measured in duplication using the Human TIMP-(1-4) Magnetic Luminex Performance 4-plex kit LKTM003 (R&D Systems, Inc, Minneapolis, MN, USA), which was designed for the simultaneous quantitative determination of the concentrations of multiple TIMPs in a single sample in cell culture supernates, serum, plasma, saliva, urine, and human milk. The Magnetic Luminex Performance 4-plex Kit LKTM003 assay was calibrated against highly purified recombinant human TIMPs produced at R&D Systems. Bio-Plex Manager 6.1 (Bio-Rad Lab Inc, Hercules, CA, USA) was used for the creation of 5-log standard curves, curve fitting, and calculation of concentrations for all analyses. Determinations of biological samples were performed in a certified hospital laboratory.
REFERENCE GROUP:
The reference group consisted of 10 healthy volunteers (5 men, 5 women) with an average age of 50.6 (±9.6) years and a negative history of kidney and other serious diseases. Concentrations of serum TIMP-1-4 and urine TIMP-1-2 were measured in this group as in the study group, but only once.
BIOETHICAL TRANSPARENCY:
This study was approved by the authorized Bioethical Committee at the Military Institute of Medicine – National Research Institute (approval No. 36/WIM/2015). All performed techniques followed the currently applicable regulations of conducting research projects. Patients recruited to the study group and volunteers from the control group provided voluntary written consent for participation in this research. They had complete insight into the project objectives, were informed about its progress, and had the opportunity to withdraw at any stage of the investigation.
STATISTICAL ANALYSIS:
For crude data, the results were presented as medians (range), due to the non-symmetrical distribution. For comparisons of the studied parameters on each day with the reference values, the one-sample Wilcoxon test was applied. For comparisons of the studied parameters on each day between AKI and non-AKI status, the exact Mann-Whitney U test was used. To investigate the relationship between studied parameters, time from injury, and AKI status, generalized linear mixed models (GLMM) for repeated measurements were estimated. The interaction term was taken into account, to reflect the possible differences in the course of studied parameters in relation to AKI. A gamma probability distribution of the error term, log link function, and first-order autoregressive covariance structure were assumed based on the Akaike information criterion. Asymmetry of distributions and the need for comparability between estimated and crude data were taken into account by using the gamma probability. The effect of risk factors on hospitalized patients was measured by mean values with 95% confidence intervals (CI) as a function of the number of days from injury and AKI status.
A
Results
CHARACTERISTICS OF THE STUDY GROUP:
The study included 33 adult patients (22 men, 11 women) with an average age of 48 (±18.58) years, and with BMI and TBSA values in the upper limits of the norm for the Polish population. Table 1 presents the general characteristics of the study group.
TIMP-1-4 CONCENTRATION VALUES AND AKI RISK:
The observed individual median concentration values of TIMP-1-4 are presented in Table 2, depending on AKI status (AKI and non-AKI), number of days of observation that had elapsed since the injury, and their relationship with the reference values.
The mean values of TIMP-1-4 in blood serum (sTIMP-1-4) and TIMP-1-2 in urine (uTIMP-1-2) estimated using GLMM are presented in Table 3, depending on the AKI status and the number of days since injury.
Figures 1 to 4 show the estimated mean and 95% CI calculated in the multivariate GLMM model for TIMP-1-4 concentrations within the first 5 days after burn injury.
The average values of sTIMP-1 and uTIMP-1 were significantly higher than the reference values (Tables 2, 3; Figure 1A, 1B). Generally, sTIMP-1 values were higher than those of uTIMP-1, and the tendency to decrease was slower. In instances of positive AKI status, the dynamics of sTIMP-1 and uTIMP-1 value changes were approximately parallel. High amounts persisted during the first 1 to 2 days, and subsequently, there was a decrease toward values comparable with non-AKI status; however, in urine this process was faster.
No relationship between sTIMP-1 concentration and the number of elapsed days since the injury and AKI risk was demonstrated in the analysis for multiple measurements. However, a significant relationship between uTIMP-1 concentration and AKI occurrence (P=0.037) was shown. A significantly higher uTIMP-1 concentration on day 1 after injury in instances of AKI (P=0.021) was also confirmed (Table 3).
The average concentration of sTIMP-2 in the study group remained below the reference group values during the entire period of observation (Tables 2, 3; Figure 2A). In AKI status, sTIMP-2 tended to slowly decrease during all the days of observation. In instances of non-AKI status, the levels of sTIMP-2 were more stable, but no significant differences between the results obtained during AKI and non-AKI status were found. However, in the analysis of multiple measurements, no association between sTIMP-2 concentration and the number of days that had elapsed since injury and AKI occurrence was found (Table 3).
The dynamics of uTIMP-2 value changes throughout the time of observation differed from those of sTIMP-2 values. Alterations of uTIMP-2 concentration in AKI instances, as well as non-AKI, were irregular and were generally above reference values, especially in AKI-positive status (Tables 2, 3; Figure 2B). In the analysis of multiple measurements, no relationship between uTIMP-2 concentration and the number of days that had elapsed since injury and AKI occurrence was found (Table 3).
The average values of sTIMP-3 in the study group remained mostly above the reference values, especially in AKI-positive status. Significantly higher activity in instances of AKI-positive status than in AKI-negative status were also confirmed in the first days after injury (P=0.016 on day 1, P=0.013 on day 2; Tables 2, 3; Figure 3). Additionally, the relatively strong relationship between sTIMP-3 and AKI occurrence was confirmed in the analysis of multiple measurements (P<0.001), but no association between sTIMP-3 concentration and the number of days that had elapsed since injury was shown (Table 3).
The maintained high activity of sTIMP-4 in AKI-positive status in comparison to non-AKI status, and the values of reference concentrations in the first 4 days after injury were visualized in our observations. The average concentrations of sTIMP-4 in AKI and non-AKI status were similar on days 3 to 5, reaching values close to the average reference concentration. The results have a tendency toward a slight increase during the first 4 days in non-AKI status (Tables 2, 3; Figure 4).
The relationship between sTIMP-4 and AKI risk was not confirmed, but significantly higher concentrations of sTIMP-4 in the first days after injury in AKI instances (P=0.019 on day 1, P=0.028 on day 2) were confirmed in the analysis for multiple measurements (Table 3).
Discussion
TISSUE INHIBITOR OF MATRIX METALLOPROTEINASE 1:
TIMP-1 is the first discovered and best-known protein of the TIMPs group, with a molecular weight of 30 kDa [27]. It can inhibit almost all types of MMPs [28]. In a series of publications, an increase in TIMP-1 value during AKI was confirmed. In the paper by Huang et al, a link between uTIMP-1 increase and risk of AKI development and a decline in survival of children in serious condition was demonstrated [29]. Bojic et al showed a positive association between the increase in sTIMP-1 and the sepsis-associated type of AKI [30]. Ozkan et al revealed an analogous association with sTIMP-1 and uTIMP-1 in patients with heterogenic etiology of AKI [31]. However, Wang et al confirmed a high value of sTIMP-1 increase for sepsis prediction, severe clinical course, and patient death, but they did not show a significant relationship with risk of AKI [32].
In the present study, significantly higher values of sTIMP-1 and uTIMP-1 in comparison to the reference values were confirmed. The values of sTIMP-1 were higher than those of uTIMP-1. The tendency for the largest changes in TIMP-1 in both serum and urine during first 24 and 48 h from thermal injury was confirmed. Longer continuation of TIMP-1 activity in blood serum than in urine was also found, which was consistent with the results cited above.
Previous reports, including those with the participation of burn patients, confirmed post-burn disorders of TIMP-1 activity in response to the systemic pro-inflammatory state. Nagy et al noted an increase in sTIMP-1 from day 2 until the end of a 5-day observation period and its weak positive association with patient survival [33]. In the study by Dasu et al, higher TIMP-1 activity in children with burns, but without significant dynamics during the several days of observation, was demonstrated [34]. Although the work of Hasback et al was based on a single sTIMP-1 measurement in each patient, the obtained results are grouped in terms of the hour/day intervals from the burn. The maximization of sTIMP-1 values during the first 48 h was confirmed in the cited analysis, which is consistent with our results. Additionally, a link between TIMP increase and severity of injury and poor survival prognosis of patients was shown [35]. Ulrich et al presented a significant sTIMP-1 rise during the first 3 days in patients with severe burns treated surgically [36]. Conversely, the report by Stanciu et al describes a slow increase of sTIMP-1 up to 7 days after injury [17].
In the present study, no relationship between sTIMP-1 and the number of days since injury and AKI risk was demonstrated. Only a significant relationship between uTIMP-1 concentration and AKI occurrence and higher uTIMP-1 concentration at the closest time after injury in instances of AKI was confirmed.
However, the relationship between TIMP-1 value alterations and risk of AKI development associated with burns was not analyzed in any of the cited studies. The absence of consistent results for measurements in serum and in urine is unclear and requires further investigation.
TISSUE INHIBITOR OF MATRIX METALLOPROTEINASE 2:
TIMP-2 is a 24 kDa protein. TIMP-2 is known to form high-affinity complexes with almost all types of MMPs. TIMP-2, unlike the other TIMPs, is not inducible by growth factors. A distinctive feature of TIMP-2 is its ability to selectively regulate MMP-2 activity. TIMP-2 is the only TIMP that can both inhibit and activate MMP. The effect of TIMP-2 on MMP-2 depends on its concentration values – low amounts stimulate MMP-2 expression and high amounts inhibit MMP-2 activity. Thus, depending on the biological situation, TIMP-2 can intensify or inhibit ECM degeneration and nephroprotection processes [37,38].
Additionally, TIMP-2 has the unique potential to directly block the proliferation of endothelial cells. The anti-proliferation mechanism is associated with an exceptionally strong ability to inhibit the cell cycle in the G1 phase. This is a protective function against DNA destruction in the case of sudden cell ischemia in critical situations. It can have a positive effect in the emergency situation of ischemia-reperfusion injury syndrome occurrence by restraining secondary tissue destruction after reperfusion. Similar activity is also presented by insulin-like growth factor binding protein 7 (IGFBP-7), and both cytokines are termed cell cycle arrest biomarkers [39].
Unfortunately, only a few papers are available that describe the prognostic sTIMP-2 value as a potential AKI marker. In the work by Wang et al, the ambiguous and dualistic role of sTIMP-2 in the AKI mechanism was indicated as being caused by simultaneously inhibiting MMPs (especially MMP-2) and promoting their synthesis in the gene transcription phase [40].
The most specific and characteristic features of sTIMP-2 during the entire period of observation were its values below the reference values. The sTIMP-2 values in AKI-positive status, similarly to that of sTIMP-1, tended to slowly decrease throughout the days of observation. In non-AKI instances, the sTIMP-2 levels presented a similar tendency but were more stable.
This is probably related to the unique ability of TIMP-2 to alternate the possibility of MMP-2 stimulation/inhibition, which is characterized by one of the strongest potentials for ECM remodeling. It is well known that higher TIMP-2 values (observed in the first days) inhibit MMP activity, protectively impacting ECM and decreasing the risk of destruction. The decrease in activity in the further part of observation can indicate a rising tendency of MMP-2 stimulation to initiate remodeling and remove damaged ECM elements, potentially reducing the risk of organ fibrosis. However, no association between sTIMP-2 concentration and the number of elapsed days since the injury and AKI occurrence was confirmed in the present study.
The association between increase of uTIMP-2 or uTIMP-2*IGFBP-7 product and risk of AKI development was described in recent publications. This applied to AKI with post-contrast etiology (Sun et al), septic etiology (Molinari et al, Kashanii et al), after sudden cardiac arrest (Adler et al), postoperative (Wang et al), and posttraumatic (Sakyi et al) etiologies [41–45]. However, studies presenting uTIMP-2 alone or together with uIGFBP-7 in burn patients are limited. Only a few reports showing the utility of these biomarkers in early prediction and diagnosis of AKI in high-risk patients with various injuries, including burns, are available [46].
The dynamics of uTIMP-2 differed from those of sTIMP-2 in the present study. The values of uTIMP-2 were more variable and above reference values, especially during the entire time of observation in AKI-positive status. The increase in levels to the maximal amounts on day 3 was noticeable. This is probably associated with the hypothesis that renal tubular cells are the main source of uTIMP-2 synthesis and secretion, as presented in the previously cited study by Kashani et al. Disintegration of interstitial cells in response to post-thermal damage of nephrons causes rapid TIMP-2 release in the renal tubular lumen and an increase in concentration in urine [39]. However, the link between the increase of uTIMP-2 and the risk of AKI shown in this publication was relatively weak and not statistically significant. Additionally, no relationship between uTIMP-2 and the number of elapsed days since injury and AKI occurrence was shown.
TISSUE INHIBITOR OF MATRIX METALLOPROTEINASE 3:
TIMP-3 is expressed in various human tissues. The molecular weight of TIMP-3 is about 24 kDa [47]. TIMP-3 is unique among the TIMPs because of its broad inhibitory range. It can deactivate almost all types of MMPs, including a number of ADAMs (a disintegrin and metalloproteases), and ADAMTS (ADAM with thrombospondin motifs) [48]. TIMP-3 can not only inhibit the activated form of MMPs but can also interrupt the promotion of pro-enzymes. TIMP-3 can also modify the angiogenesis process through suppression of vascular endothelial growth factor [49]. TIMP-3 is the only one from the TIMP group that does not exist in a soluble form, so it occurs only in the ECM and basal membranes [50].
The level of TIMP-3 is relatively high in healthy kidney tissue. Its decrease can be observed during tubulointerstitial fibrosis [51]. The link between decreased TIMP-3 concentrations and a greater risk of renal interstitial damage was shown in the study by Wang et al. However, the interpretation of these observations is still unclear. The authors emphasized the nephroprotective impact of TIMP-3, resulting from blocking MMP-2 synthesis and secretion, and subsequently rapid nephron fibrosis inhibition [44]. Daniels et al described the positive effect of TIMP-3 on the return to normal kidney function after AKI, and a reduction in demand for renal replacement therapy was demonstrated in their publication. The authors related this finding to the strong suppression of kidney inflammation and fibrosis [52]. Similarly, Zhou et al showed the influence of increased TIMP-3 activity on risk reduction of AKI with an ischemic mechanism. The authors justified this by the especially strong inhibition of MMP-2 and MMP-9 [53].
The values of sTIMP-3 in the study group remained mostly above the reference values in the present study. Instances of AKI-positive status were also significantly higher than that of AKI-negative status. This was likely related to the potent TIMP-3 action described above, which suppressed the impact of multiple MMPs. These enzymes are well-known strong stimulators of post-burn inflammation. Additionally, a relevant relationship between sTIMP-3 and AKI occurrence was shown, but with no association between sTIMP-3 and the number of days from injury. Unfortunately, no data dealing with the role of TIMP-3 in the course of burns were found in the available literature. However, judging by the results of the presented work and the references cited above, potential benefits of TIMP-3 evaluations in the diagnostics of post-burn AKI can be expected.
TISSUE INHIBITOR OF MATRIX METALLOPROTEINASE 4:
TIMP-4 is the last and weakest known member of the TIMP family. Its molecular weight is about 25.5 kDa. The TIMP-4 molecule shows the greatest similarity in structure to TIMP-2. The essential difference between TIMP-4 and TIMP-2 concerns the C-terminal domain sequence, determining the unique influence of MMP-2 activity. This is the cause of the similar bioactive properties of TIMP-4 and TIMP-2, but only within the scope of MMP inhibition [54].
In our observations, high activity of sTIMP-4 in AKI-positive status in comparison with non-AKI status and the values of reference concentrations were observed, especially just after the time of injury. Comparing the graphs of sTIMP-4 and sTIMP-2 (Figures 2A, 4), a specific analogy in the course of the concentration curves of AKI/non-AKI during the entire period of observation could be seen. However, the sTIMP-2 results reached values on average around 100 times higher than those of sTIMP-4. Additionally, the sTIMP-2 and sTIMP-4 result curves were positioned differently than those of the reference data. This was probably associated with the unique TIMP-2 feature, which was based on the induction capabilities of MMPs in low-concentration conditions. However, a significant relationship between sTIMP-4 and AKI risk was not confirmed.
SUMMARY OF TIMPS:
A similar configuration could be seen in the distribution of all types of TIMP data. The AKI-positive agents generated the highest TIMP values. The non-AKI status values were localized mostly between AKI-positive and reference curves. The reference values were situated at the bottom of the charts. The only exception was the case of sTIMP-2, for which a mirror inversion could be seen; this was probably connected with the unique ability of TIMP-2 to not only inhibit but also to promote the MMP activities.
Although statistical significance was not confirmed in all cases and types of TIMP, the differences between values in AKI status could be clearly seen. The increased level of blood serum and urine TIMPs could be treated as a useful AKI marker after burn injury.
Also worth mentioning is the mutual relationship between the AKI-positive, AKI-negative, and reference values. The maximum discrepancy could be seen mostly in the first 48 h after the injury. In the subsequent days, the courses of the graph curves became closer to each other, nearly overlapping at the end of the observation time.
This confirms that the time of maximum TIMP storm occurs during the first 48 h after the burn injury. During this time, their potential power as AKI biomarkers seems to be the greatest. This is likely the best moment for intensive testing of these markers in the blood serum and urine to improve the AKI diagnostics. The levels of cut-off points for the increase of TIMPs should be carefully standardized. This can be a goal for future investigations. The greatest limitation is the lack of wide-ranging publications describing this important clinical problem.
STUDY LIMITATIONS:
The small number of patients affected by massive thermal injuries during the project period did not allow us to prove the existence of all observed relationships. However, statistical power of 60% to 70% was obtained when testing the significance of the associations. Also, the different times from the moment of thermal injury to the first TIMP evaluation appeared to be a serious technical problem, which resulted in different time intervals for the first evaluation. To account for this fact, mixed longitudinal models were used. Finally, the activities of TIMP-3-4 were analyzed only in blood serum. None of the certified laboratory tests validated for measurements of these parameters in the urine were achievable at the time of implementation of the project.
Conclusions
TIMPs seem to play an important role during the early phase of AKI processes in patients with severe burns as indicators of damage to the nephrons’ ECM. Systemic evaluations of TIMPs, both in blood and in urine, have potential benefits and improve AKI diagnostics, being helpful in assessing the risk of its occurrence at an early stage. The important roles of uTIMP-1 and sTIMP-3, and their relationships with AKI were confirmed. They can be considered as the potential novel markers of AKI risk in the first days after thermal injury. Analyses of other possible associations of TIMPs require further studies with a larger cohort of patients, taking into account measurements of uTIMP-3 and uTIMP-4.
Figures
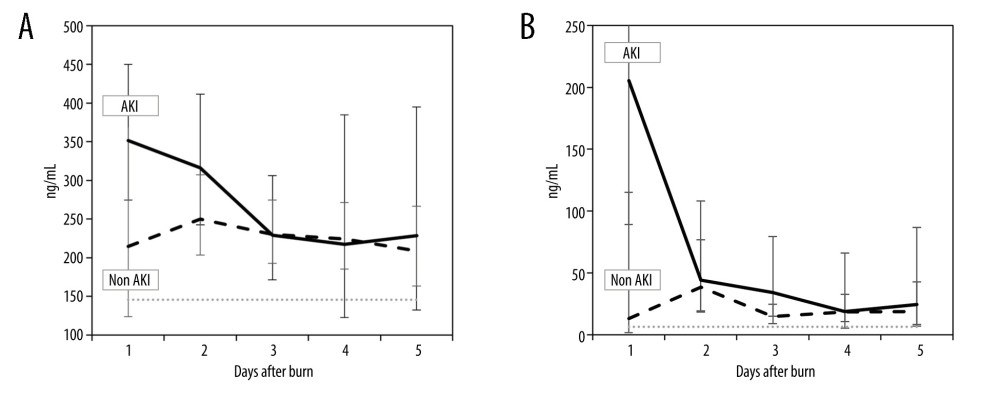 Figure 1. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-1 (TIMP-1) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-1; (B) uTIMP-1. Dotted line indicates the reference value.
Figure 1. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-1 (TIMP-1) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-1; (B) uTIMP-1. Dotted line indicates the reference value. 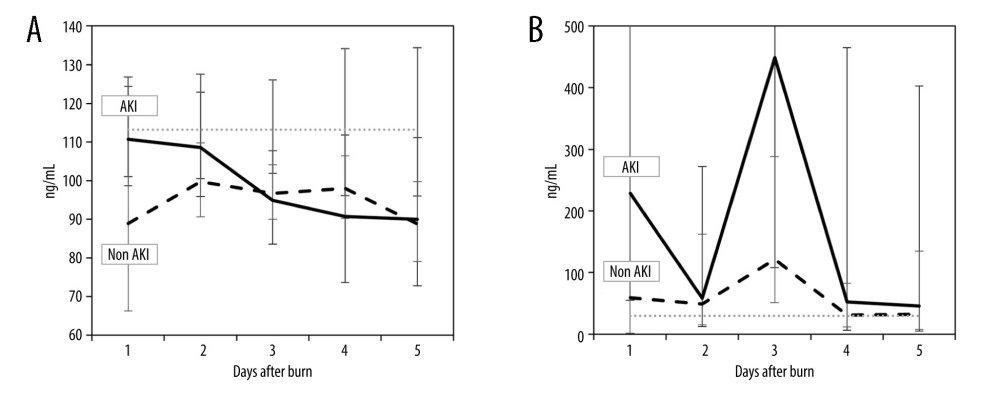 Figure 2. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-2 (TIMP-2) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-2; (B) uTIMP-2. Dotted line indicates the reference value.
Figure 2. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-2 (TIMP-2) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-2; (B) uTIMP-2. Dotted line indicates the reference value. 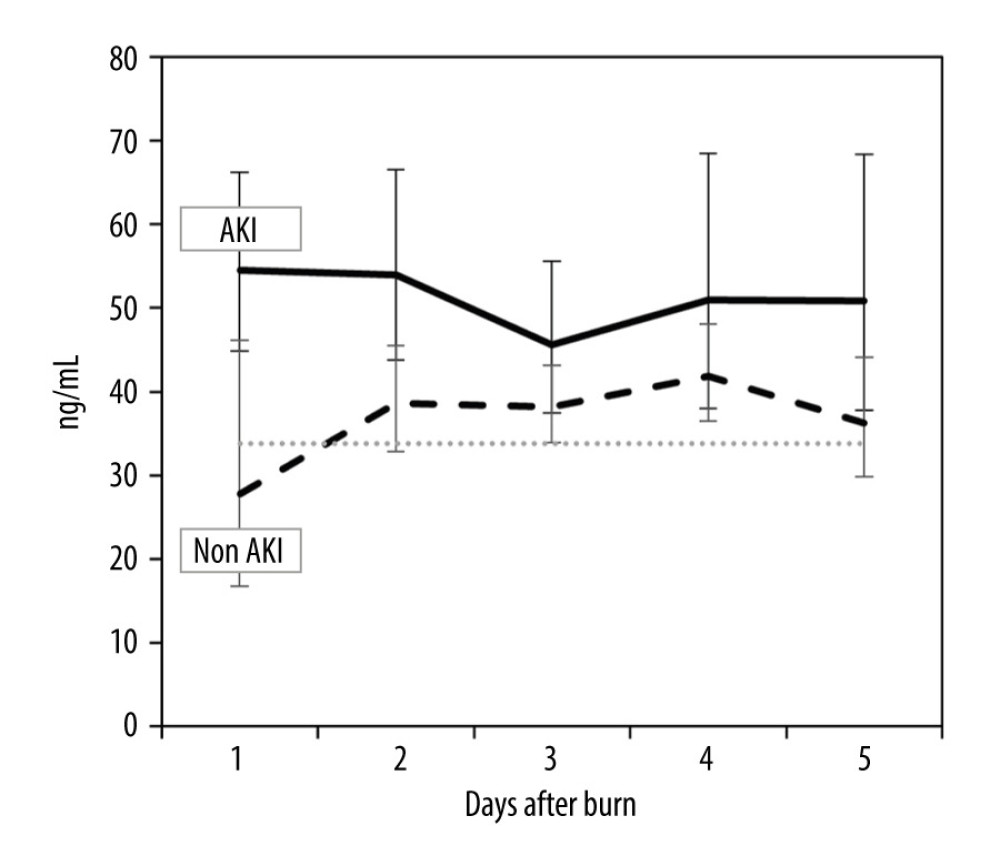 Figure 3. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-3 (sTIMP-3) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value.
Figure 3. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-3 (sTIMP-3) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value. 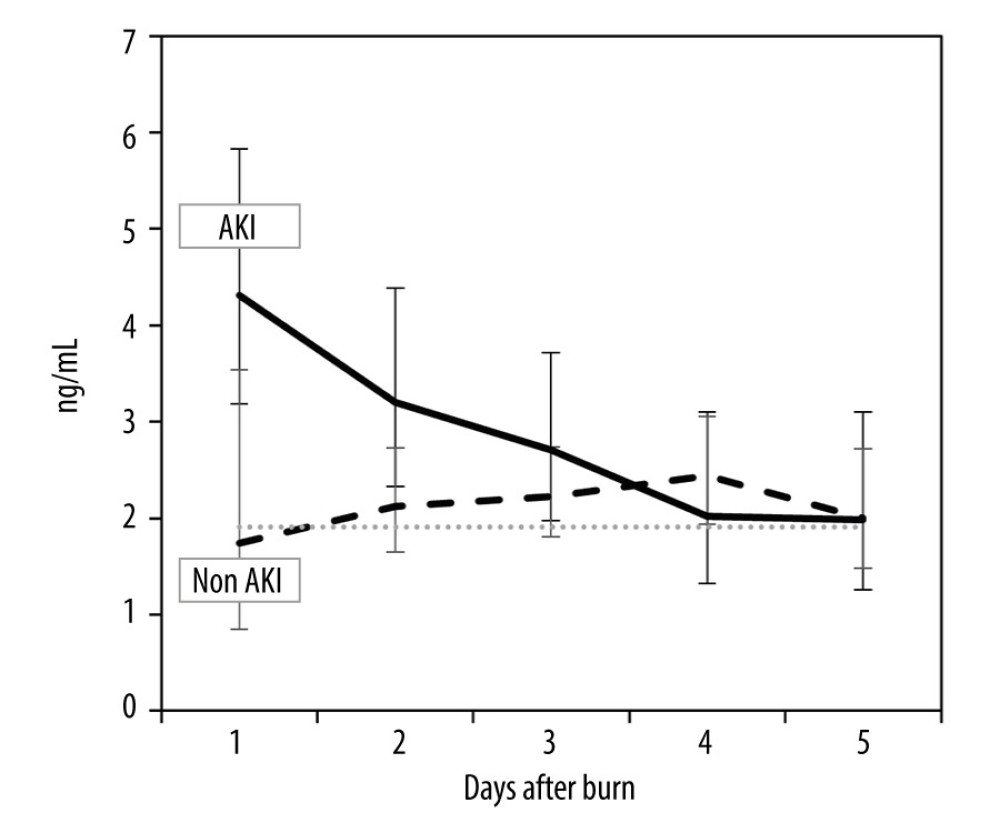 Figure 4. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-4 (sTIMP-4) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value.
Figure 4. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-4 (sTIMP-4) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value. References
1. Witkowski W, Kawecki M, Surowiecka-Pastewka A, Early and late acute kidney injury in severely burned patients: Med Sci Monit, 2016; 22; 3755-63
2. Oudemans-van Straaten HM, Circulating pro-apoptotic mediators in burn septic acute renal failure: Crit Care, 2008; 12(2); 126
3. Kaushal GP, Haun RS, Herzog C, Metalloproteinase and its role in acute kidney injury: Am J Physiol Renal Physiol, 2013; 304(9); F1150-58
4. Sharma C, Dobson GP, Davenport LM, The role of matrix metalloproteinase-9 and its inhibitor TIMP-1 in burn injury: A systematic review: Int J Burns Trauma, 2021; 11(4); 275-88
5. Young PK, Grinnell F, Metalloproteinase activation cascade after burn injury: A longitudinal analysis of the human wound environment: J Invest Dermatol, 1994; 103; 660-64
6. Fuller BJ, Ischaemia/reperfusion injury and inflammation: Transplantation, 2000; 69(3); 327-28
7. Catania JM, Chen G, Parrish AR, Role of matrix metalloproteinases in renal pathophysiologies: Am J Physiol Renal Physiol, 2007; 292; F905-F11
8. Sampieri CL, Orozco-Ortega RA, Matrix metalloproteinases and tissue inhibitors of metalloproteinases in chronic kidney disease and acute kidney injury: A systematic review of the literature: Hippokratia, 2018; 22(3); 99-104
9. Kunugi S, Shimizu A, Kuwahara N, Inhibition of matrix metalloproteinases reduces ischemia-reperfusion acute kidney injury: Lab Invest, 2011; 91(2); 170-80
10. Yang X, Chen C, Teng S, Urinary matrix metalloproteinase-7 predicts severe AKI and poor outcomes after cardiac surgery: J Am Soc Nephrol, 2017; 28(11); 3373-82
11. Fu H, Zhou D, Zhu H, Matrix metalloproteinase-7 protects against acute kidney injury by priming renal tubules for survival and regeneration: Kidney Int, 2019; 95(5); 1167-80
12. Basu RK, Donaworth E, Siroky B, Loss of matrix metalloproteinase-8 is associated with worsened recovery after ischemic kidney injury: Ren Fail, 2015; 37(3); 469-75
13. Kaneko T, Shimizu A, Mii A, Role of matrix metalloproteinase-2 in recovery after tubular damage in acute kidney injury in mice: Nephron Exp Nephrol, 2012; 122(1–2); 23-35
14. Raeeszadeh-Sarmazdeh M, Do LD, Hritz BG, Metalloproteinases and their inhibitors: Potential for the development of new therapeutics: Cells, 2020; 9(5); 1313
15. Arpino V, Brock M, Gill SE, The role of TIMPs in regulation of extracellular matrix proteolysis: Matrix Biol, 2015; 44–46; 247-54
16. Schrezenmeier EV, Barasch J, Budde K, Westhoff T, Schmidt-Ott KM, Biomarkers in acute kidney injury – pathophysiological basis and clinical performance: Acta Physiol (Oxf), 2017; 219(3); 554-72
17. Stanciu AE, Zamfir-Chiru-Anton A, Stanciu MM, Role and dynamics of matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 in burn patients: Exp Ther Med, 2021; 22(4); 1062
18. Novak KB, Le HD, Christison-Lagay ER, Effects of metalloproteinase inhibition in a murine model of renal ischemia-reperfusion injury: Pediatr Res, 2010; 67(3); 257-62
19. Stander M, Wallis LA, The emergency management and treatment of severe burns: Emerg Med Int, 2011; 2011; 161375
20. Mulder PPG, Vlig M, Boekema BKHL, Persistent systemic inflammation in patients with severe burn injury is accompanied by influx of immature neutrophils and shifts in T cell subsets and cytokine profiles: Front Immunol, 2021; 11; 621222
21. Brew K, Nagase H, The tissue inhibitors of metalloproteinases (TIMPs): An ancient family with structural and functional diversity: Biochim Biophys Acta, 2010; 1803(1); 55-71
22. Fuller BJ, Ischaemia/reperfusion injury and inflammation: Transplantation, 2000; 69(3); 327-28
23. Hu Q, Lan J, Liang W, MMP7 damages the integrity of the renal tubule epithelium by activating MMP2/9 during ischemia-reperfusion injury: J Mol Histol, 2020; 51(6); 685-700
24. Covington MD, Bayless KJ, Burghardt RC, Ischemia-induced cleavage of cadherins in NRK cells: Evidence for a role of metalloproteinases: Am J Physiol Renal Physiol, 2005; 289(2); F280-88
25. Caron A, Desrosiers RR, Béliveau R, Ischemia injury alters endothelial cell properties of kidney cortex: Stimulation of MMP-9: Exp Cell Res, 2005; 310(1); 105-16
26. Kunugi S, Shimizu A, Kuwahara N, Inhibition of matrix metalloproteinases reduces ischemia-reperfusion acute kidney injury: Lab Invest, 2011; 91(2); 170-80
27. Batra J, Robinson J, Soares AS, Matrix metalloproteinase-10 (MMP-10) interaction with tissue inhibitors of metalloproteinases TIMP-1 and TIMP-2: Binding studies and crystal structure: J Biol Chem, 2012; 287(19); 15935-46
28. Vandenbroucke RE, Libert C, Is there new hope for therapeutic matrix metalloproteinase inhibition?: Nat Rev Drug Discov, 2014; 13(12); 904-27
29. Huang H, Lin Q, Dai X, Derivation and validation of urinary TIMP-1 for the prediction of acute kidney injury and mortality in critically ill children: J Transl Med, 2022; 20(1); 102
30. Bojic S, Kotur-Stevuljevic J, Kalezic N, Diagnostic value of matrix metalloproteinase-9 and tissue inhibitor of matrix metalloproteinase-1 in sepsis-associated acute kidney injury: Tohoku J Exp Med, 2015; 237(2); 103-9
31. Ozkan H, Okuturlar Y, Koçoğlu H, Serum levels and urinary excretion of Tenascin-C and TIMP-1 in acute kidney injury: Clin Lab, 2019; 65(10); 190233
32. Wang M, Zhang Q, Zhao X, Diagnostic and prognostic value of neutrophil gelatinase-associated lipocalin, matrix metalloproteinase-9, and tissue inhibitor of matrix metalloproteinases-1 for sepsis in the Emergency Department: An observational study: Crit Care, 2014; 18(6); 634
33. Nagy B, Szélig L, Rendeki S, Dynamic changes of matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 after burn injury: J Crit Care, 2015; 30(1); 162-66
34. Dasu MR, Spies M, Barrow RE, Herndon DN, Matrix metalloproteinases and their tissue inhibitors in severely burned children: Wound Repair Regen, 2003; 11(3); 177-80
35. Hästback J, Fredén F, Hult M, Matrix metalloproteinases −8 and −9 and tissue inhibitor of metalloproteinase-1 in burn patients. A prospective observational study: PLoS One, 2015; 10(5); e0125918
36. Ulrich D, Noah EM, von Heimburg D, Pallua N, TIMP-1, MMP-2, MMP-9, and PIIINP as serum markers for skin fibrosis in patients following severe burn trauma: PlastReconstr Surg, 2003; 111(4); 1423-31
37. Fan W, Ankawi G, Zhang J, Current understanding and future directions in the application of TIMP-2 and IGFBP7 in AKI clinical practice: Clin Chem Lab Med, 2019; 57(5); 567-76
38. Hernandez-Barrantes S, Toth M, Bernardo MM, Binding of active (57 kDa) membrane type 1-matrix metalloproteinase (MT1-MMP) to tissue inhibitor of metalloproteinase (TIMP)-2 regulates MT1-MMP processing and pro-MMP-2 activation: J Biol Chem, 2000; 275(16); 12080-89
39. Kashani K, Al-Khafaji A, Ardiles T, Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury: Crit Care, 2013; 17(1); R25
40. Wang Z, Famulski K, Lee J, TIMP2 and TIMP3 have divergent roles in early renal tubulointerstitial injury: Kidney Int, 2014; 85(1); 82-93
41. Sun Q, Kang Z, Li Z, Xun M, Urinary NGAL, IGFBP-7, and TIMP-2: Novel biomarkers to predict contrast medium-induced acute kidney injury in children: Ren Fail, 2022; 44(1); 1201-6
42. Molinari L, Del Rio-Pertuz G, Smith AProCESS and ProGReSS-AKI Investigators, Utility of biomarkers for sepsis-associated acute kidney injury staging: JAMA Netw Open, 2022; 5(5); e2212709
43. Adler C, Heller T, Schregel F, TIMP-2/IGFBP7 predicts acute kidney injury in out-of-hospital cardiac arrest survivors: Crit Care, 2018; 22(1); 126
44. Wang Y, Zou Z, Jin J, Urinary TIMP-2 and IGFBP7 for the prediction of acute kidney injury following cardiac surgery: BMC Nephrol, 2017; 18(1); 177
45. Sakyi SA, Ephraim RKD, Adoba P, Tissue inhibitor metalloproteinase 2 (TIMP-2) and insulin-like growth factor binding protein 7 (IGFBP7) best predicts the development of acute kidney injury: Heliyon, 2021; 7(9); e07960
46. Niculae A, Peride I, Tiglis M, Burn-induced acute kidney injury-two-lane road: From molecular to clinical aspects: Int J Mol Sci, 2022; 23(15); 8712
47. Wick M, Härönen R, Mumberg D, Structure of the human TIMP-3 gene and its cell cycle-regulated promoter: Biochem J, 1995; 311(Pt2); 549-54
48. Fan D, Kassiri Z, Biology of tissue inhibitor of metalloproteinase 3 (TIMP3), and its therapeutic implications in cardiovascular pathology: Front Physiol, 2020; 11; 661
49. Qi JH, Ebrahem Q, Moore N, A novel function for tissue inhibitor of metalloproteinases-3 (TIMP3): Inhibition of angiogenesis by blockage of VEGF binding to VEGF receptor-2: Nat Med, 2003; 9(4); 407-15
50. Arpino V, Brock M, Gill SE, The role of TIMPs in regulation of extracellular matrix proteolysis: Matrix Biol, 2015; 44–46; 247-54
51. Casagrande V, Federici M, Menghini R, TIMP3 involvement and potentiality in the diagnosis, prognosis and treatment of diabetic nephropathy: Acta Diabetol, 2021; 58(12); 1587-94
52. Daniels JR, Ma JZ, Cao Z, Discovery of novel proteomic biomarkers for the prediction of kidney recovery from dialysis-dependent AKI patients: Kidney360, 2021; 2(11); 1716-27
53. Zhou X, Zang X, Guan Y, Targeting enhancer of zeste homolog 2 protects against acute kidney injury: Cell Death Dis, 2018; 9(11); 1067
54. Melendez-Zajgla J, Del Pozo L, Ceballos G, Maldonado V, Tissue inhibitor of metalloproteinases-4. The road less traveled: Mol Cancer, 2008; 7; 85
Figures
Figure 1. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-1 (TIMP-1) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-1; (B) uTIMP-1. Dotted line indicates the reference value.Figure 2. Estimated means and 95% CI for serum (s) and urine (u) tissue inhibitor of metalloproteinase-2 (TIMP-2) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). (A) sTIMP-2; (B) uTIMP-2. Dotted line indicates the reference value.Figure 3. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-3 (sTIMP-3) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value.Figure 4. Estimated means and 95% CI for serum tissue inhibitor of metalloproteinase-4 (sTIMP-4) concentrations during first 5 days since burn injury by acute kidney injury status (Microsoft Excel, Microsoft 365 MSO). Dotted line indicates the reference value. Tables
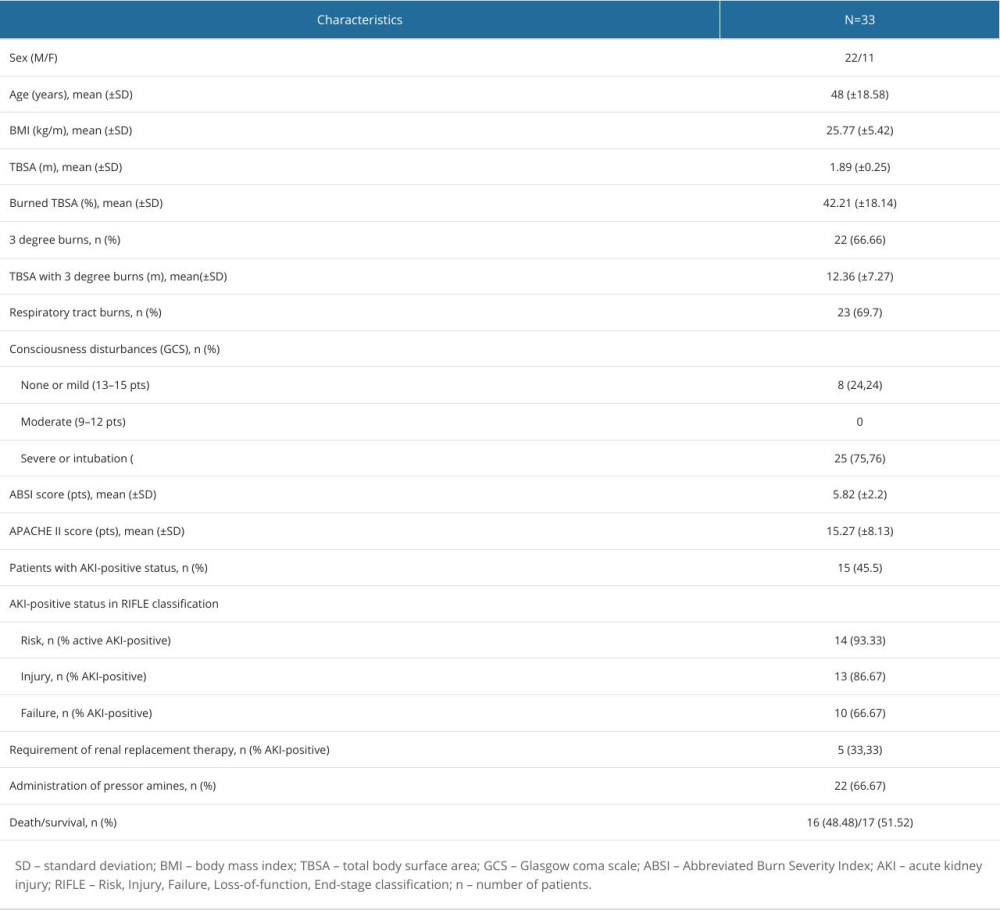 Table 1. Characteristics of the studied group of patients.
Table 1. Characteristics of the studied group of patients.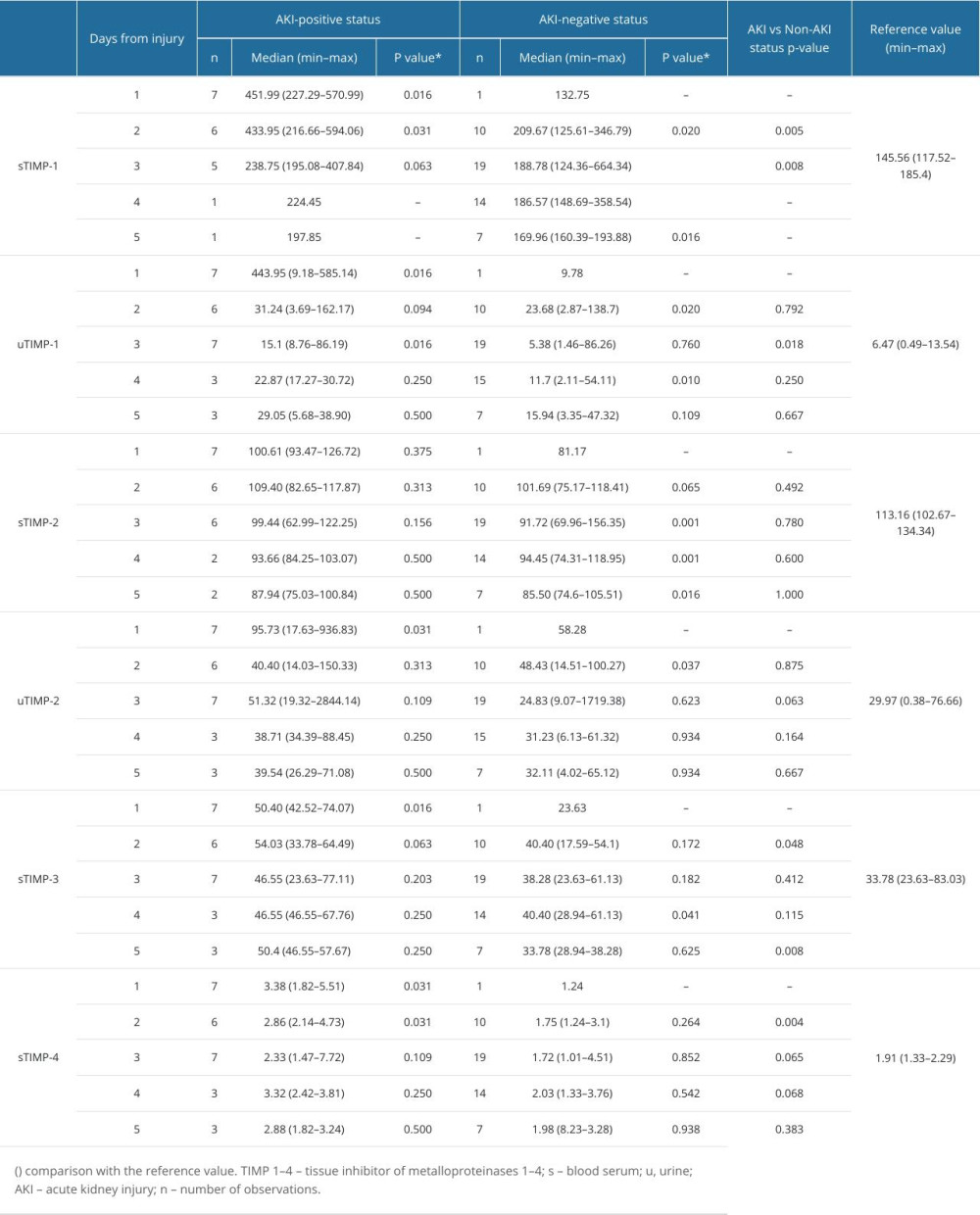 Table 2. TIMP-1-4 concentration values (ng/mL) obtained during the observation period.
Table 2. TIMP-1-4 concentration values (ng/mL) obtained during the observation period.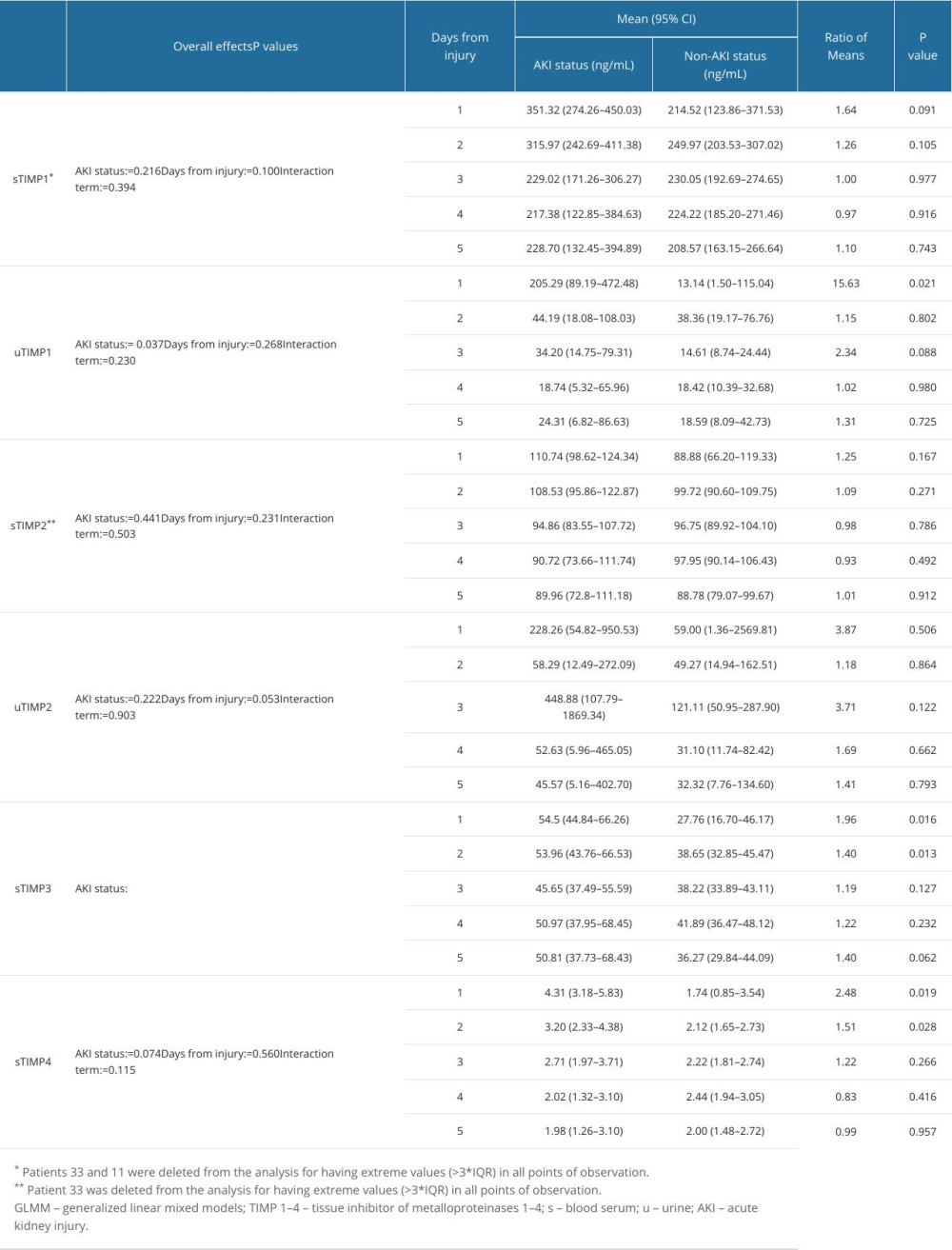 Table 3. Estimated means of TIMP-1-4 parameter concentrations with acute kidney injury status and the number of days from injury (GLMM model).Table 1. Characteristics of the studied group of patients.Table 2. TIMP-1-4 concentration values (ng/mL) obtained during the observation period.Table 3. Estimated means of TIMP-1-4 parameter concentrations with acute kidney injury status and the number of days from injury (GLMM model).
Table 3. Estimated means of TIMP-1-4 parameter concentrations with acute kidney injury status and the number of days from injury (GLMM model).Table 1. Characteristics of the studied group of patients.Table 2. TIMP-1-4 concentration values (ng/mL) obtained during the observation period.Table 3. Estimated means of TIMP-1-4 parameter concentrations with acute kidney injury status and the number of days from injury (GLMM model). In Press
26 Mar 2024 : Clinical Research
New Computerized Planning Algorithm and Clinical Testing of Optimized Nuss Bar Design for Patients with Pec...Med Sci Monit In Press; DOI: 10.12659/MSM.943705
07 May 2024 : Clinical Research
Treatment of AVN-Induced Proximal Pole Scaphoid Nonunion Using a Fifth and Fourth Extensor Compartmental Ar...Med Sci Monit In Press; DOI: 10.12659/MSM.944553
16 Mar 2024 : Clinical Research
Diagnostic Efficiency of ACR-TIRADS Score for Differentiating Benign and Malignant Thyroid Nodules of Vario...Med Sci Monit In Press; DOI: 10.12659/MSM.943228
08 May 2024 : Clinical Research
Effect of Individualized PEEP Guided by Driving Pressure on Diaphragm Function in Patients Undergoing Lapar...Med Sci Monit In Press; DOI: 10.12659/MSM.944022
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952